
Hayward Study Guide Hematology
Case of elderly female with melena and dark bloody emesis with a hgb of 9. Teaching point was to transfuse prbc’s based on the patient’s condition rather than just the number. Harwood and Elise comments: We have had it beaten into our heads to not transfuse unless the hgb is <7. This question makes the point that you also need to consider the patient’s clinical status. If the patient has life threatening bleeding, it is reasonable to initiate transfusion prior to a hgb of 7.
Petechiae is the most common sign of ITP. Acute ITP is more common in kids. Chronic ITP more common in adults.

Differentiating severe liver disease from DIC is difficult but the d-dimer should be normal or only minimally elevated with severe liver disease.
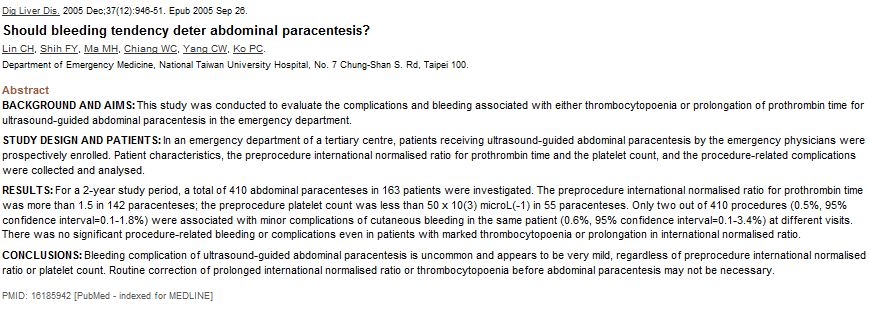
There is debate regarding doing a paracentesis with a platelet count less than 20 or an INR >2. Elise comment: There is controversy on this topic. Elise would be ok with doing a paracentesis with an INR <4. Christine agreed. Elise comment: Elise found a study of over 1000 paracentesis and many patients had an INR of around 2 or platelet count less than 50 and all did well.
Quick medline search also found this abstract:
Most commonly observed abnormality with DIC is thrombocytopenia. Most common cause of DIC is gram negative sepsis.
Hemophilia patient with a head injury needs factor 8 replacement prior to any imaging. Elise comment: this is critical knowledge for both real life and the boards. Girzadas comment: Patients will often come in with their own factor 8.
Von Willebrand DZ with gingival bleeding can be treated with DDAVP intranasally. Avoid NSAIDs in patients with von willebrand dz.
Acute chest syndrome is the leading cause of death in patients with sickle cell disease in the US. Hydroxyurea can decrease the incidence of painful crises in adults but is not approved for pediatric patients.
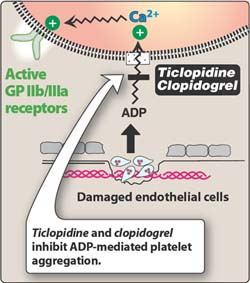
Clopidagrel inhibits the ADP receptor on the platelet.
ABO transfusion reaction results in hemoglobinemia and hemoglobinuriauria, decreased serum haptoglobin, elevated ldh. In one series of reports, the combination of an increased serum LDH and a reduced haptoglobin was 90 percent specific for diagnosing hemolysis, while the combination of a normal serum LDH and a serum haptoglobin >25 mg/dL was 92 percent sensitive for ruling out hemolysis. Haptoglobin binds to Hgb released during intravascular or extravascular hemolysis. (Up to Date)
Febrile neutropenic patients: You should avoid rectal exam if you can. Harwood comment: the only time I would do a rectal in such a patient is if the patient has a fever and complains of rectal pain. Any other complaints, I don’t do a rectal. Elise comment: I totally agree.
Finger tip laceration on a patient with INR of 6: Harwood comment: Stitch it up, apply pressure dressing and give oral vitamin K (2.5mg). Girzadas comment: For skin avulsion of finger tip, apply heme-con and give oral vitamin K. Elise comment: New recommendations from American College of Chest Surgeons says no oral vitamin K in the non-bleeding patient unless the INR is 10 or higher.
Up to Date Chart for Management of Supratheraputic INR. They lean toward the 2008 guidelines in that they still suggest vitamin k for non-bleeding patient with INR between 5 and 10. Again the ACCP 2012 guidelines recommend no vitamin k for non-bleeding patients with INR’s less than 10.

Treatment of hypercalcemia: Initial treatment is normal saline IV to restore euvolemia. Aggressive hydration and lasix has fallen out of favor because it does not lower calcium more than saline alone. Next step is calcitonin. Steroids may be useful with some tumors.
Managing sickle cell pain crises: Elise comment: new thinking is avoid fluid boluses and just give maintenance fluids. Excess fluids may result in atelectasis or acute chest syndrome. Consider using D5.45 because normal saline may increase sickling. Also no benefit to O2 unless patient is hypoxic. Oral rehydration is also acceptable.
Treatment for TTP is plasma exchange.
Wise Morbidity and Mortality (some details changed so specific case is not identifiable)
Teenage female was hit by an auto. Obvious head trauma with altered mental status. Pt is intubated on arrival. After tracheal intubation, pt desaturates and becomes bradycardic. Pt had left chest needle thoracostomy placed with rush of air from the left chest. Subsequently vitals improved. Presumed diagnosis was tension pneumothorax. Team was next concerned about head injury, pulmonary contusions, possible intra-abdominal injury, and open right humerus fracture.
Pt was sent directly to the PICU following CT imaging. This was done based on neurosurgery concerns about intracranial injury. Neurosurgery wanted the patient up in the ICU to have a intracranial pressure monitoring device placed. Harwood comment: I don’t feel this was the right decision by the ED to let this patient go up to the PICU at this point in the workup.
When patient gets to PICU, the results of the abdomen/pelvis CT shows severe pelvic fx with pelvic hematoma. Pt becomes hypotensive in PICU. She is basically an unstable peds trauma patient in the PICU. Patient was started on dopamine and IV fluids. Hgb was 6. PRBC transfusion was started. Patient was too unstable to go to IR. Peds Ortho Attending took patient to OR to place ex-fix of pelvis.
Opportunity for improvement: Don’t let a patient out of the ED environment until the patient is stabilized even if a consultant is saying to send the patient up to the PICU now. We should review critical tests prior to sending patient from ED to another unit.
No strong evidence that intracranial pressure monitoring improves outcomes in kids.
Harwood: A type and cross and PRBC’s generally should be ordered in ED. Pelvic fx can be identified and management begun in ED by wrapping pelvis. Prioritizing the head injury over the torso injuries risks missing life-threatening injuries. The torso injuries are what are going to kill a polytraumatized young person. Dopamine is generally not indicated to manage hypotension in trauma patients. PRBC’s and IV crystalloid are standard management of hypotension in trauma patients . Kids/teenagers can maintain a normal range bp until they crash. You gotta watch the pulse because that will show early hypotension before the blood pressure will. Central lines are generally not critical to trauma resuscitations. Large bore peripheral IV’s and Intraosseous lines can provide crystalloid and blood products probably faster. Elise comment: Trauma resuscitations are different than medical resuscitations and in general should be done in the ED not the ICU.
Adjust your trauma algorithm for kids/teenagers. Speak calmly and softly to them. Do not give direct orders to them.
Thoracic trauma accounts for 20% of pediatric trauma deaths. Kids have a compliant chest wall and can have serious injuries of chest and abdomen without fx. Ribs provide less protection for liver and spleen. Use broslow tape to determine chest tube size in younger children.
Abdominal wall is less developed and less protective. Kidneys more prone to fracture. Spleen has a strong capsule and is less likely to rupture.
Pediatric Trauma score: (higher the better/less than 8 has 20% mortality and needs transfer to trauma center) Our patient had a score of 4.
Pediatric Trauma Score
|
Components |
+2 |
+1 |
-1 |
SCORE |
|
Weight |
>20 kg (44 lbs) |
10-20 kg (22-44 lbs) |
<10 kg (22 lbs) |
|
|
Airway |
Patent |
Maintainable |
Unmaintainable |
|
|
Systolic BP Pulses |
> 90 Radial |
50 – 90 Carotid |
< 50 Nonpalpable |
|
|
CNS |
Awake |
+LOC (responsive) |
Unresponsive |
|
|
Fractures |
None |
Closed or suspected |
Multiple closed or open |
|
|
Wounds |
None |
Minor |
Major, penetrating or Burns > 10% |
|
|
TOTAL SCORE |
|
|||
|
9 –12 Minor Trauma Use local guidelines/protocols 6 –8 Potentially Life Threatening Suggests need for Trauma Center 0 –5 Life Threatening Need for Trauma Center <0 Usually Fatal Transport to Nearest Facility |
||||
Mckean comment: Sometimes with trauma and non-trauma patients, the ER is the best place for them for awhile. We have the specialized knowledge/skill and access to rapid diagnostic testing that is not available in any other area of the hospital. Tekwani comment: We need to overcome our own anxiety as physicians with these traumatized kids/teenagers and understand we are the best people to manage them in the hospital. Harwood comments: If you see tire marks on the torso, you have to proceed under the assumption that there are internal injuries. However, at times you will be amazed how kids and adults can have body parts get run over by cars and not have any injury. Every patient has an end point when it is reasonable for them to go up to the unit. Key thing is to identify the life threatening injuries and begin addressing their management in the ED. After that, the ICU can continue management.
McKean CPC Case Presentation for the National Championship at ACEP in Seatle
4yo child with altered mental status. Developed on a plane ride home from Walt Disney World. Pt was noted to have left side weakness. Ct showed right sided hypodense lesions. Angiogram shows carotid dissection on right. It was thought child suffered dissection from roller coaster ride. Pt was treated with ASA and did well.
Kettaneh My right leg is cold ( some details altered so specific case is not identifiable)
79 yo male with cold right leg and abdominal pain. Pt has RLQ tenderness and absent pulses in the right leg below femoral pulse (femoral pulses present bilat). Vascular surgery consulted immediately. Heparin started. Dissection was clinically ruled out by the presence of bilaterally equal femoral pulses. Harwood comment: Heparin is problematic prior to evaluating for AAA. Kettaneh: Pt had an ultrasound done at the bedside showing a normal abdominal aorta. Treatment for arterial occlusion is heparin, asa, iv fluids, pain control, dependent positioning of affected limb. Labs in this case showed acutely decreased gfr, elevated cpk and elevated lactate, and leukocytosis. ED physicians ordered CT abdomen to evaluate abdominal pain/ abnormal labs. Prior to CT aabd/pelvis however, pt went to the OR for vascular surgery thrombectomy. The night after surgery, pt developed peritonitis. CTA showed ischemic bowel, renal infarcts and thrombus in the aorta. There was some note of an intimal flap in the aorta. Patient died. Although this patient was likely not salvageable even at ED presentation, again this case brings up the issue that the ED has the global picture of the patient and needs to identify critical diagnoses before giving the patient up to the management of the consultant.
Knight FEIBA for the Rapid Reversal of Bleeding in Patients with Warfarin Induced Coagulopathy
FFP for reversal has the limitations of large volume, incomplete reversal, and need for type and cross match.
FEIBA is basically a 4 factor prothrombin complex concentrates
We gave FEIBA and IV vitamin K to reverse warfarin coagulopathy in patients with major hemorrhage (life/limb threat, intracranial bleed, drop of 2 HGB).
Time to INR of 1.5 or less was 127 minutes. 4 patients died (19%). 4 patients had thrombotic complications after day 3 following FEIBA for a rate of 14%. This rate of thrombotic events is higher than previous studies. FEIBA’s duration of action is 72 hours so these thromboses may be due to the patient no longer being anticoagulated rather than the effect of FEIBA. Elise and Harwood comments: there is risk of thromboses from underlying pathology and being in the ICU. Those risks are likely more the cause of thrombotic events in these patients rather than FEIBA
Katiyar McGurk Sayger Documentation/Coding for Medical Decision Making
Medical decision making section: Provides a capsule summary of what is going on with this patient and the direction of management.
3 categories that make up medical decision making: # of possible diagnoses, amount of data/diagnostic testing that was analyzed, risk of significant morbidity/mortality.
It is not enough to say I reviewed a test. You have to say what your interpretation is of the test.
Document for example: pt presents with fever, cough and sob. Will evaluate with cxr, cbc, chemistries abg and blood cultures. Will initiate treatment with nebulized albuterol.
Document what you learned from review of prior records.
Document your discussions with consultants and pmd.
Document your discussion with family members.
Document re-evaluation of patients. Include if you utilized a specific guideline like PERC or Heart Score.
Ryan Med Student Review