
Bolton GI Emergencies Study Guide
Erythema nodosum is associated with inflammatory bowel disease.
Most common cause of bacterial diarrhea presenting to the ED is campylobacter. Viruses are still the most common cause of diarrhea overall. You can use anti-motility agents to improve patients’ symptoms of diarrhea.
Pepto bismal taken QID and prophylactic antibiotics can reduce the incidence of traveler’s diarrhea but it is not recommended in a normal healthy traveller. Resistance to Cipro is increasing when used to treat traveller’s diarrhea. Elise comment: Is cipro still the drug to take with you on a trip? Molly’s response: yes it is still first line for traveller’s diarrhea . Elise checked the CDC website and indeed, cipro is still recommended for first line management of traveller’s diarrhea.
Emphysematous Cholecystitis is a rare but dangerous disease process. It requires aggressive resuscitation and surgical management. ED Antibiotics need to cover anaerobes and gram negatives.
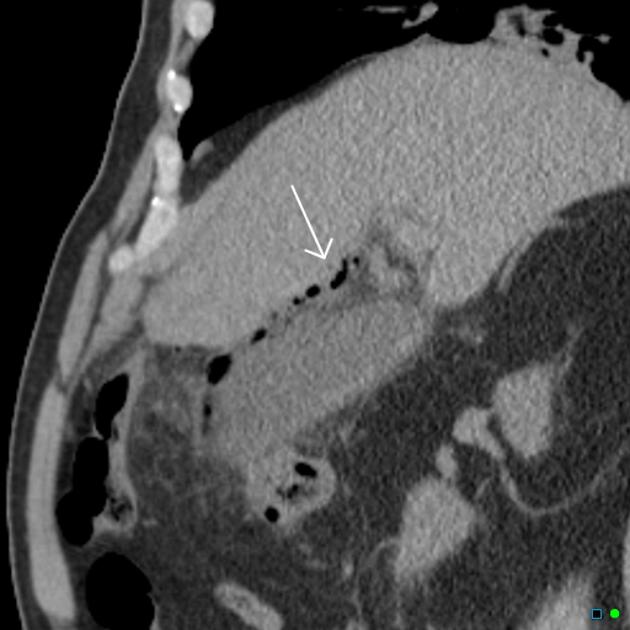
*Emphysemaous Cholecystitis (google image)
Toxic Megacolon needs to be treated with IV fluids, broad spectrum antibiotics, and IV steroids. Probably prudent to discuss steroid administration and dosing with GI consultant.
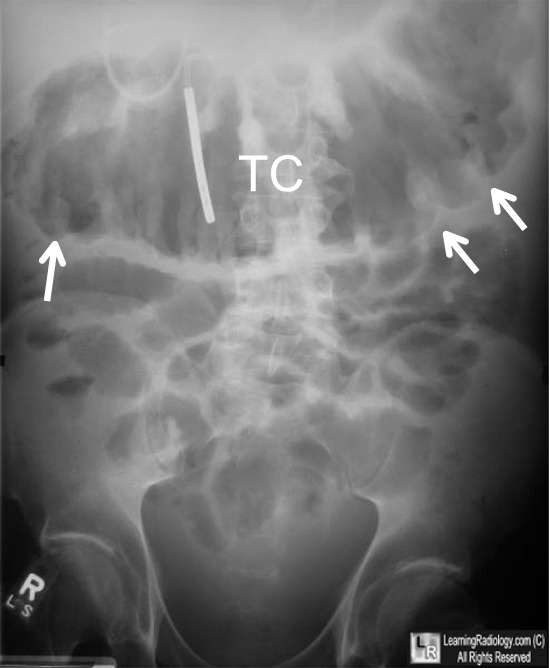
*Toxic Megacolon (google image) Note large width of tranverse colon and thumb-printing
Epigastric pain that improves with food and worsens in the middle of the night suggests PUD. Epigastric pain that worsens with food suggests gastritis
Crohn’s disease carries risk of retroperitoneal abscess and fistula. Faculty comment: Great teaching point, this could be missed easily in clinical practice. Molly discussed a case in a patient with history of crohn’s and vague back pain and limp who had a psoas abscess.

*Chron’s disease with psoas abscess (google image)
Porcelain gallbladder increases patient’s risk of gallbladder cancer.
Sonographic criteria for cholecystitis: wall thickness >3mm, pericholecystic fluid, CBD >7mm, positive sonographic murphy’s sign
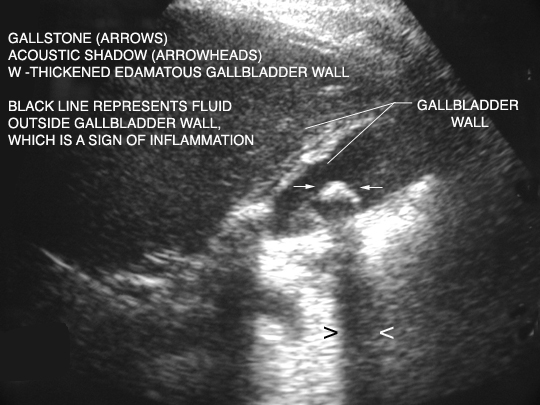
*U/S of Cholecysitis (google image)
Flagyl is first line therapy for C-Diff colitis. Oral therapy is preferred. If C-diff recurs you should initially attempt a second course of Flagyl and if that fails oral vancomycin is the next choice C-Diff is a toxin mediated diarrhea. C-Diff can develop even after a short course of antibiotics.
H.pylori irradication decreases the incidence of recurrent PUD down to the 15% range.
Crohn’s disease lesions tend to extend through all layers of the bowel. UC lesions tend to be limited to the mucosa.
15% of cholecystitis is acalculous. More common in elderly patients and ICU patients.
Coins in the esophagus will lie with the coin “en face” on the PA view. In kids, the coin will get stuck in the proximal esophagus in the area of the cricopharyngeous (usually around the calvicles). Button batteries in the esophagus have even more urgency to have them removed. Resident comment: I have seen two button batteries removed from the esophagus and both children had burns in their esophagus within 1.5 hours.

*Coin in the esophagus (google image)
Infectious complications of pancreatitis usually develop 5-15 days after onset of pain.
Epiploic appendigitis is caused by torsion of an epiploic appendage (basically an epiploic appendage is a stalk of blood vessel/tissue/adipose/serosal surface hanging from the colon and projecting into the peritoneal cavity). Treatment is supportive and it usually resolves in about 2 weeks. Patients do not need surgery for this disease process. Clinically it can look very similar to appendicitis.
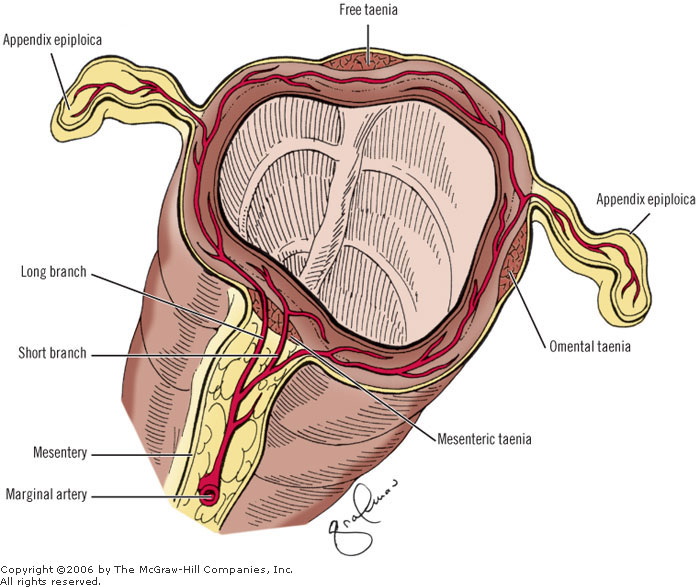
*epiploic appendage (google image)

*Ranson Criteria for Pancreatitis (google image)
Boerhaave’s syndrome: full thickness perforation of esophagus, usually due to vomiting, requires broad spectrum antibiotics and surgery, it carries a high mortality.
Ogilvie syndrome is a colonic pseudo-obstruction. Treat with neostigmine and or erythromycin ( both stimulate colonic activity) and/or decompression with colonoscopy.
*Ogilvie syndrome (google image)
Most common cause of esophageal perforation is iatrogenic.
Most common cause of small bowel obstruction is adhesions. #2 is hernia. Girzadas comment: If a patient has a small bowel obstruction and they don’t have surgical scar on their abdomen, look for a hernia. I have made the mistake of admitting a patient with an undiscovered incarcerated inguinal hernia.
Mesenteric Ischemia: CT abdomen/pelvis with IV contrast has 64% sensitivity for mesenteric ischema.. CT angio is diagnostic modality of choice with higher sensitivity than usual CT . Mortality of mesenteric ischemia is 50% if diagnosed in first 24 hours
Febbo/Gupta Oral Boards
Case 1. 84yo male presents with syncope and hypotension. Patient is uncomfortable and is incontinent of stool. EKG shows paced rhythm with sgarbossa criteria for STEMI. CXR shows very large heart. Diagnosis: Cardiogenic shock due to Inferior wall MI Critical actions: Identify shock, fluid resuscitation, pressor support, cath lab activation. Gupta comment: use ultrasound at the bedside to rule out other causes of shock such as pericardial fluid, AAA, tension pneumothorax, valve rupture, PE, wall rupture.
Case 2. 24yo male presents requesting drug detox. Pt has low grade temp. He also feels sob and fatigued and has a cough. On physical exam patient has oral thrush. Diagnosis: PCP pneumonia Critical actions: Recognize clinical picture of HIV with cough/dyspnea, treat with Bactrim and steroids. Gupta comment: ABG with Po2 <70 indicates need for steroids.
Case 3. 25yo female presents with dyspnea. Patient has history of pyoderma gangrenosum Diagnosis: Methemoglobinemia due to dapsone treatment pyoderma gangrenosum Critical actions: methylene blue administration. Andrea comment: If a patient taking dapsone has a G6PD deficiency, methylene blue can worsen the hemoglobinemia. If a patient with methemoglobinemia from dapsone has anemia consider that they could have a G6PD deficiency and consider giving them a transfusion prior to giving them methylene blue.
Carlson Anticholinergics and TCA’s
Anticholinergics predominantly affect the muscarinic receptors rather than the nicotinic receptors.
Anticholinergic toxidrome: Blind as a bat, red as a beet, hot as Hades, dry as a bone, mad as a hatter., blurred vision, vasodilation, elevated temperature, dry skin/mouth/mucous membranes/arm pits, urinary retention, CNS depression/excitation/hallucinations.
Less common features include seizures, arrhythmias, coma, hypotension, rhabdomyolysis.
In patients with anticholinergic symptoms from antihistamine overdose, check also for acetaminophen overdose. Many medications contain combinations of Benadryl and Tylenol. Also check for ASA.
Anticholinergic Overdose Management: Manage agitation with benzodiazepines. Avoid beta-blockers and calcium channel blockers. Treat QRS prolongation/WCT with bicarb or lidocaine. Physostigmine is a pure antidote to anticholinergics. Physostigmine is a carbamate which is a reversible acetylcholinesterace inhibitor. Average duration of physostigmine is 60 minutes but most anticholinergic drugs have an effect for several hours. So , if patients improve with physostigmine they need to be observed for 4-6 hours to see if the anticholinergic symptoms recur. Indications for physostigmine are pure anticholinergic overdose and: coma, intractable seizures, severe agitation, or symptomatic narrow complex tachydysrhythmia. There is still a lot of concern about giving physostigmine. There are 1980’s case reports about fatal outcomes when given in setting of TCA overdose. There has been some revisionist thinking about physotigmine lately and now it is considered more user/patient friendly. Still, avoid it in the setting of TCA overdose, poly-drug overdose and with wide complex tachycardia.
Recent case report discussed the fact that topical atropine eye drops have 150 mg of atropine in a full bottle. The bioavailability of topical atropine drops is 60%. So this has potential for serious toxicity and possibly as a Mcgyver type antidote in the hospital if we ran out of regular atropine. Resident comment: If there was a nerve gas exposure to a large group of people and the hospital ran out of atropine, you could have patients drink atropine eye drops. Andrea agreed this was a reasonable idea.
Night shade is an anticholinergic plant. It has a bunny ears leaf. Mandrake is another anticholinergic plant.

*night shade leaf (google image)
TCA’s are “dirty drugs”, they have multiple effects on the body. Anticholinergic, alpha blockade, gaba blockade, Na and K channel blockade, H1/H2 receptor blockade effects.
Clinical picture: Tachycardia, QRS prolongation, Terminal R wave widening in AVR, brugada patern, QT prolongation, bradycardia/asystole, hypotension, seizures, coma,
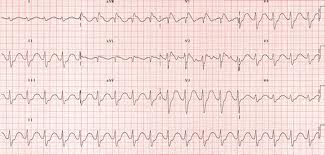
*TCA EKG (google image) note wide terminal R wave in AVR, tachycardia and widened QRS
Treatment for TCA overdose: Sodium bicarb is indicated for QRS >110, marked acidosis, refractory hypotension, cardiac arrest. Push 1 amp at a time. You can also hang a bicarb drip. Be sure to monitor the patient’s potassium. Second line antiarrythmic is lidocaine (1b agent). You want to avoid 1a and 1c agents.

*antiarrythmic classification (google image)
Seizures are frequently self limited in TCA overdose but first line treatment is benzodiazepines. Second line treatmet for seizures is propofol. There are some case reports suggesting intralipid may be helpful. Avoid flumazenil, physostigmine, 1a/1c antiarrythmics and beta/calcium channel blockers in TCA overdose.
TCA overdose disposition: If asymptomatic after 6 hours, they are medically clear for admit for psychiatric evauation. If patient has persistent tachycardia, admit for OBS. Any other signs admit the patient to the ICU.
Beckemeyer Seizure Management
First line: Lorazepam. Second line: phenytoin. Third line: Phenobarb or Keppra or Valproic acid.
Intubation may be indicated when giving multiple anti-seizure meds. Especially when using benzo’s and phenobarb. If you have to use a neuromuscular blocker for a prolonged time you may need to have the patient on continuous EEG monitoring.
Consider pyridoxine for refractory seizures (INH overdose antidote)
Purple glove syndrome can occur from multiple doses of phenytoin in elderly patients. This is not from a IV malfunction or extravasation into the soft tissues. Harwood and Elise comment: This is likely due to propylene glycol.

*purple glove syndrome (google image)
Febrile seizures: Occurs between 3months and 6 years of age, generalized seizure, last less than 15 minutes. Child is back to normal shortly after seizure. Faculty discussion about work up indicated for febrile seizures: Most agreed that if child can be observed to be normal per parents within an hour after seizure they don’t need an LP. They just need an appropriate work up for source of fever (exam, +/- UA and CXR) In younger kids (<6 months) there may be some lower threshold to LP because it is more difficult to assess mental status/return to baseline.
Harwood comment: I don’t get any labs other than anti-seizure drug level in patients with known history of seizure disorder who present to the ED with an acute seizure.
Elise comment: Get a CT for trauma, fever, immunocompromise, change in seizure type, history of cancer, warfarin use, or focal neuro deficit.
Paik Follow Up Lecture
49yo male with 2 months of jaundice and weight loss. Pt has abdominal distension and hepatomegaly. CT shows ascites and cirrhotic liver. Patient was admitted from the ED. 20 days later he presents to the ED again. This time he has hematemesis and hypotension. Patient received protonix and octretide in the ED. He was admitted to ICU. EGD showed portal hypertension with no active bleeding.
Management for Active hematemesis: Protonix, Octreotide, IV antibiotics, infusion of blood products, vitamin K, consider sangstoken-blakemore tube, consult GI consultant to scope patient emergently and or consult IR to perform TIPs procedure.
Dr. Paik discussed the technique of placing the Blakemore tube. A key point is that hanging a bag of saline from the outer portion of the tube will apply adequate pressure on the stomach balloon. Bonder comment: IV antibiotics have a low NNT for improving patients with upper GI bleed. IV ceftriaxone is a reasonable choice but probably any antibiotic coverage of gram negatives is effective
Parker Follow Up Lecture
Pt presented with respiratory distress due to aspiration pneumonitis. Pt was in hospice but was placed on bipap in the ED. CXR showed cardiomegaly and vascular congestion. Pt improved clinically and bipap was discontiued. Pt worsened and bipap was re-started. Pt stabilized and was admitted. Pt deteriorated on the floor and family made decision to withdraw bipap treatment. Pt died on the floor.
Aspiration is primarily a chemical pneumonitis. 26% have superimposed bacterial infection. Do not treat with empiric antibiotics. Provide suctioning and positive pressure ventilation as needed. No steroids.
Elise and Christine comment: Don’t give empiric antibiotics to relatively healthy patients with simple aspiration. Treat only if patient develops CXR infiltrate with signs of pneumonia. Add clindamycin to standard CAP regimen and Zosyn to standard HAP regimen.
Nevin High Reliability Organizations
HRO’s operate under very trying conditions yet manage to have fewer than their share of accidents. HRO’s attempt to make systems ultra safe
Facts about errors: everyone makes them, most serious events are due to systems or process problems.
Diagnostic Errors: Framing, obedience to authority, premature closure, and anchoring. Healthcare workers need to work with a questioning attitude to avoid these errors.
Most health care workers make 6.8 errors per hour. Most serious errors that reach the patient got through 9 potential stop points.
Variation is the enemy of quality.
200% accountability= 2 team members continually cross checking each other.
ARCC=Ask a question, Request a change, voice a Concern, invoke Chain of Command. This is a protocolized way of raising a concern.
SBAR is a structured way to hand off care: Situation, Background, Assessment, Recommendation.
Errors should not be a cause for blame but starting point for discussions/investigations for discovering what went wrong.
‘Why hospitals should fly” is a good book to read regarding patient safety/HRO
Dr. Nevin then discussed the new Rural EM elective rotation being offered at Bromenn Medical Center.