
Hart & Regan Wound Management
Strategies to lessen the pain of injection of local anesthetic: small gauge needle, slow injection, inject through wound margin (not intact skin), buffer with bicarb, warm to body temp, and pre-treat with topical anesthetic such as LET. Harwood comment: Use an Insulin syringe initially. It has a 31 gauge needle. Then use the longer 27guage needle to anesthetize more deeply.
Pasturella strains from cat bites are felt to be more virulent than pasturella strains from dog bites. Additionally, cats have smaller, sharper teeth that can puncture more deeply further increasing the risk of infection.
Care of Amputated digit: Wrap the digit in saline soaked gauze, place the wrapped digit in a plastic bag, place the bagged/wrapped digit on ice. Finally, keep the digit with the patient on the patient cart so the digit does not get lost.
Fight bite wounds are high risk for infection. Examine all fight bite wounds through full ROM of the MCP joint to check for tendon injury. Give Augmentin or Unasyn as initial antibiotic if patient is not penicillin allergic. Consult with Hand Surgery. If there is evidence of extensor tendon injury, joint penetration, infection, or fracture, the patient should be considered for admission for washout.

To release skin entrapment in a zipper, you need to get sturdy wire cutters or a bolt cutter to cut the median bar of the zipper. Dennis Ryan comment: This can be a tough procedure to get the median bar cut.

For lacerations around the eye, emergency physicians should probably not be repairing lacerations around the medial canthus, involving the lid margin, or if you see exposed fat. If you identify any of these, you needto consult ophthomology.

When can packing after I and D be removed? When purulence has stopped draining.
Wound VAC's work by decreasing edema, improving vacular and lymphatic flow, decreasing bacterial density and increasing granulation tissue.
Ohl/Yappo CPC Presentations
I did not want to divulge the cases because they will be presented at CORD this month.
Lorenz 5 Slide Follow UP
Patient presents with dizziness. EKG shows polymorphic ventricular tachycardia (Torsades)

The patient was alert and talking only because he had an LVAD. Patient was initially given IV magnesium without effect. Patient was next defibrillated into sinus rhythm. In hospital patient was treated with amiodarone and AICD.
Data shows that 2 year survival with an LVAD is about 23%. LVAD's can give patients a longer life. On the other hand, patientsmay experience challenges and complications from an LVAD. This risk/benefit balance was discussed.
Harwood comment: If you see a patient with torsades who does not have an LVAD you need to defibrillate and also start magnesium and an anti-arrhythmic. These patients will continue to revert to torsades after defibrillation until you get therapuetic levels of an anti-arrhythmic.
Wing 5 Slide Follow Up
Myasthenic crisis can be precipitated by infection, pregnancy, and medications (aminoglycosides, flouroquinolones, beta blockers, and magnesium).
Evaluate the patient with a measurement of Vital Capacity and NIF. Normal VC should be around 3L (bad is around 1.5L). Normal NIF should be around -60(bad is around -20). If the NIF is -20 neuro may use plasma exchange. Harwood would intubate if NIF is worse than -20.
Treatment is prednisone, IVIG, and plasma exchange. Intubation for respiratory support.
Faculty comments: Respiratory therapy can measure both VC and NIF in the ED.

Nejak STEMI Equivalents
Dan's recommended steps to evaluating an EKG: Get an old EKG to compare. Look at AVL for isolated depression. Check for loss of precordial T wave balance. Look for LMCA ischemia, Check for Wellen's and DeWinters signs. Check for reciprocal changes. Check for hyper-acute T waves.

Loss of precordial T wave balance


LMCA Occlusion shows diffuse ST depression and ST elevation in AVR and V1

DeWinter's ST depression in V2-5 with rocket shaped T waves and Subtle AVR ST elevation. This is an anterior STEMI equivilent and indicates LAD occlusion.

Wellen's is a sign of critical LAD stenosis. These patients should have Cardiology evaluation.
DeWeert, Stanek, Traylor Abdominal and Pelvis Trauma
There was a ton of information in this excellent lecture that I could not encapsulate into these notes. I put in a few key points made in the lecture.
Every 10 minute delay to give blood in trauma patients has an increased odds ratio of 1.27 for mortality.
Give TXA within 3 hours of initial trauma. It is safe and number needed to treat is somewhere between 7-67 to decrease mortality. Beyond 3 hours after injury, TXA increases mortality for unclear reasons.


Image shows the effect of a pelvic binder to close down the potential space in the pelvis. Have a low threshold to place a pelvic binder early in the course of managing a multiply injured trauma patient. There was consensus that the old strategy of "rocking the pelvis" to identify pelvic fracture on physical exam risks increasing pelvic bleeding. In the multiply injured trauma patient, bind the pelvis early on in the resuscitation, don't rock the pelvis, and get a pelvic x-ray to identify fracture.

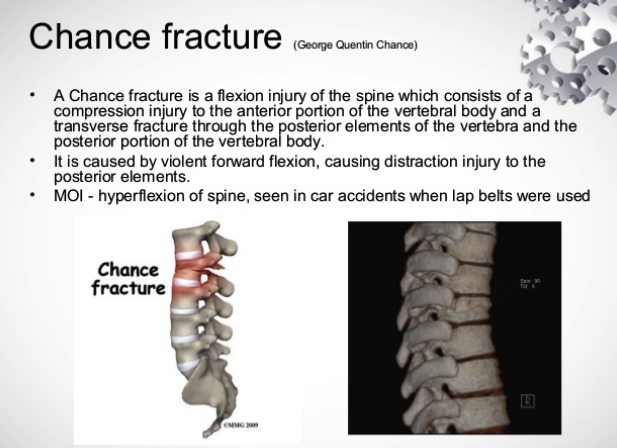
Seat belt sign is associated with increased risk of intra-abdominal injury and Chance Fracture of the lumbar spine.

Algorithm implementing FAST exam in blunt abdominal trauma

Algorithm for Blunt GU Trauma
There was a ton of information in this lecture that I could not encapsulate into these notes.